Optimizing Nerve Blocks for Orthopedic Surgery: Clinical and Billing Best Practices
One of the most significant anesthesia developments of the past 20 years is the use of nerve blocks as an adjunct anesthetic for orthopedic and abdominal procedures. The use of interscalene blocks for shoulder procedures, femoral blocks for hip procedures, sciatic blocks for back procedures and TAP blocks for abdominal procedures has increased dramatically.

This growth is driven by several factors. Many argue these blocks reduce reliance on opioids and other anesthetic agents—a key goal amid the national opioid crisis. Others point to economic benefits, particularly when blocks are used solely for postoperative pain control. Given these clinical and financial opportunities, the question is whether anesthesia practices are fully optimizing their use.
Three criteria should be considered when determining how to optimize the use of nerve blocks within your practice:
1. The requirements and preferences of the surgeon.
2. The documentation requirements of the payers.
3. The accuracy and consistency of the claims adjudication process.
Surgical considerations
Not all surgeons are proponents of nerve blocks although newer orthopedic surgeons tend to be more enthusiastic than their more seasoned colleagues. The usual concern is the administration of the block will delay the start of the case. From a compliance perspective, it is critical the surgeon agrees the anesthesia provider will perform a nerve block for purposes of postoperative pain management, and the reasons for transferring postoperative pain management to the anesthesia team are documented in the surgeon's record.
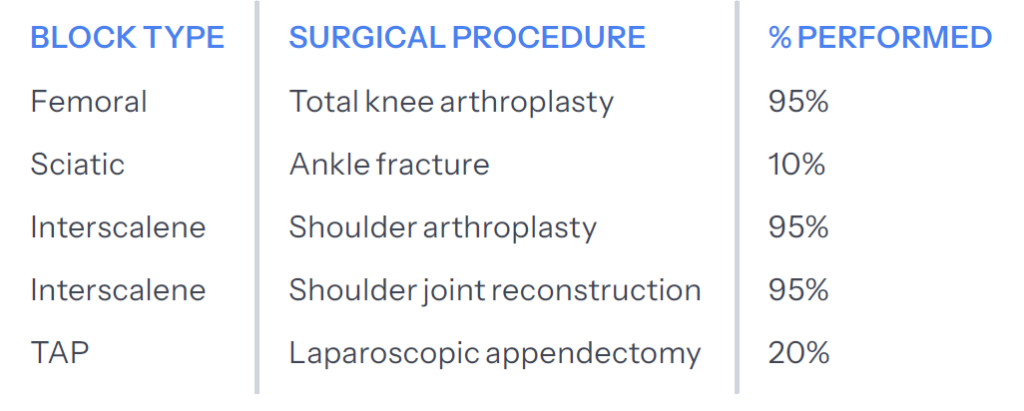
Certain procedures are especially suited for nerve blocks, with femoral and interscalene being the most common. Examples include:
Documentation requirements for billable post-op blocks
The anesthesia record must clearly confirm three elements for each postoperative pain block to be billable:
1. Block details - Who placed it, when, type (single shot or catheter, location, etc.).
2. Surgeon request - Documentation that the surgeon requested to block.
3. Post-op purpose only - Confirmation it was used solely for postoperative pain, not as part of the primary anesthetic.
Since our coding team will always confirm these criteria are met before submitting a claim, the anesthesia provider should ensure each of these elements is clearly reflected in the record.
Payer adjudication and follow-up
Even with proper documentation, claim approval is not always guaranteed. Some payers may reject block claims due to:
* Authorization or referral concerns
* Requests for additional documentation
* Modifier or coding issues
* Bundling/inclusive edits
Resolving rejections with better process
Most post-op block denials are preventable with timely follow-up and strong documentation. Key ways to improve outcomes include:
1. Standardize documentation checks before submission to prevent avoidable errors
2. Triage rejections by issue type (e.g., modifier, bundling, authorizations).
3. Set SLAs and escalation paths for timely follow-ups.
A proactive billing strategy and strong internal processes help anesthesia groups improve claim consistency and support appropriate reimbursement. Better reimbursement starts with better documentation.