
Many years ago, Mark Rogers, MD, the anesthesia chairman at Johns Hopkins, asked Robert Donham, MD, the assistant chairman, to make the operating rooms more productive, which he did. When asked about his strategy and approach, Dr. Donham explained that he had three distinct qualifications for the role. He was a board-certified anesthesiologist; he had a PhD in engineering; and he was a former Green Beret. The reality was that he had to develop a strategy to schedule cases more effectively and modify surgeon behavior, and this continues to be a major challenge for virtually every anesthesia practice.
Considering the Metrics
Measuring operating room utilization would seem to be a simple exercise involving normalized production metrics. How many cases are performed per anesthetizing location per day? The problem is that the concept of a case is not a consistent unit of production. A cursory review of any daily hospital operating room schedule clearly reveals the problem. No two cases have the same time, the same level of acuity or the same payer. This degree of specificity is often lost on hospital administrators whose primary objective is simply filling rooms with paying cases. Anesthesia providers, however, have long since learned that production is more effectively measured in time spent, units billed and the net yield per billed unit. All of this is further complicated by the manner in which cases are scheduled. While the ideal schedule includes cases evenly scheduled with consistent breaks from 7:30 AM to sometime in the later afternoon, this is often the exception rather than the rule.
The anesthesia practice incurs a cost per location by scheduling providers. When there are busy rooms with a favorable payer mix, the revenue generated covers the cost of providing the necessary service. The problem is that, as the number of anesthetizing locations increases, this is too often the exception rather than the rule. And this is why so many practices must request financial support from the facility. Historically, anesthesia practices have considered themselves impotent to change this paradigm and captive to the current case scheduling process. The good news is that many practices are starting to use their valuable database of operating room utilization data to effect meaningful change that improves the efficiency of the operating rooms and enhances the profitability of the practice.
The focus of a successful anesthesia practice should be on developing meaningful productivity measures and tracking them over time. The chart below is a typical example of room utilization at a community hospital that this client shares with administration on a monthly basis. It allows the practice to clearly identify and review staffing requirements.
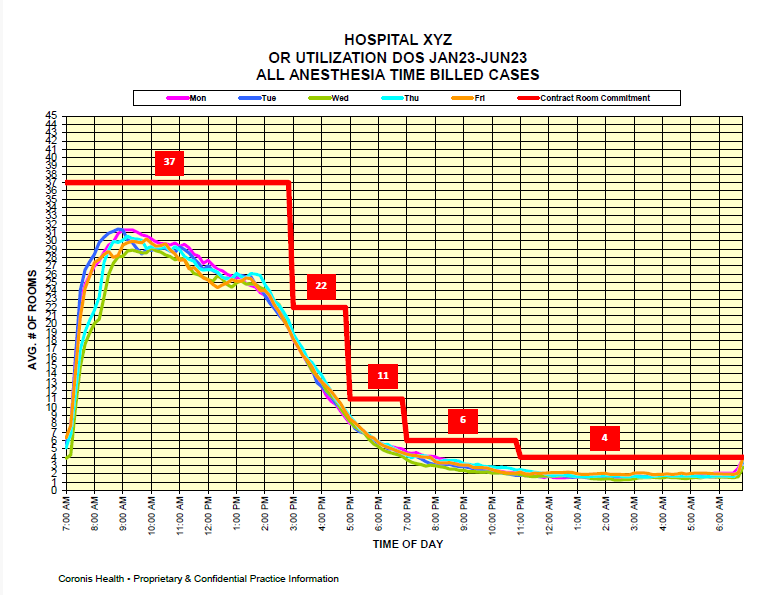
There are three standard metrics that practices monitor to assess operating room utilization. An essential requirement for all of them is the ability to identify activity either by anesthetizing location, which is most useful for care-team practices, or by provider, which is very useful for physician-only practices. Data should be normalized whether by location or provider to show average hours billed, average units billed or average yield per anesthetizing location day. Many practices prefer to divide the practice by lines of business: main OR, cardiovascular, endoscopy and outpatient. Regardless of methodology, the optimal OR utilization is 75% - 85% inclusive of turnaround time. Typically, weekends and OB are excluded from such reports or shown separately.
Managing the Matrix
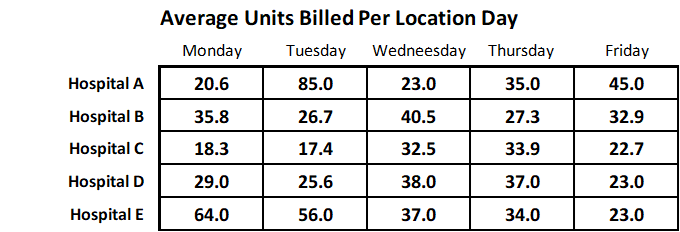
The table below shows activity from five hospitals. Each hospital ran at least 10 operating rooms per day when they were busy. The data reflects actual activity for the month of August 2023. It clearly demonstrates the variations from practice to practice and day to day. Days with an especially high value probably reflect cardiovascular cases. It may be useful to remember that a practice should generate at least 50 ASA units per eight-hour anesthetizing site that is paid at a reasonable rate per unit to cover the cost of the care.
Managing an anesthesia practice can be compared to managing an anesthetic case. Timely and reliable data is the key to effective decision-making and overall management. As in managing a case, the key is to know what the normal metrics should be so that one can make adjustments in order to get things back on track. The challenge for practice management is that there are more variables and adjusting them involves a considerably more complicated algorithm. While one can manage a case alone, managing a practice involves the whole team and administration.
As is true so often in life, traditional tools may have worked well in traditional situations; but, when things change, new tools are often required. So, it is in managing a practice. While the historical focus of practice management was revenue generation to promote profitability, today’s focus must also include cost containment via operational/staffing efficiency to yield a healthy bottom line. This requires a new set of tools and a different strategic orientation.
If you have questions about this topic, please reach out to your account executive.