
The more important question is no longer whether an anesthesiologist can produce 10,000 units annually. It is: what should productivity look like based on the care model being utilized? This is because a physician personally performing every case should not be expected to generate the same output as a physician medically directing multiple anesthetizing locations simultaneously.
Yet many organizations continue evaluating both models using the same benchmark.
Why Productivity Comparisons Often Miss the Mark
One of the biggest mistakes in anesthesia productivity analysis is treating all provider models equally. A personally performing anesthesiologist and a medically directing anesthesiologist operate fundamentally different workflows. Their daily responsibilities, room coverage and production potential are not comparable.
Still, many organizations apply one generalized productivity target across all staffing models. That creates distortion.
A physician generating approximately12,000 annual units, while personally performing, may actually be operating at a very high level. Meanwhile, another physician generating 15,000–18,000 units in a care team model may appear significantly more productive, but much of that increase reflects leverage from concurrent anesthetizing locations rather than purely individual output.
Without context, the numbers can become misleading.
Rethinking Productivity Benchmarks by Care Model
Assuming approximately eight weeks annually for vacation, holidays, CME and post-call recovery, most full-time anesthesiologists work roughly 220 clinical days per year. Using this framework, the benchmarks below represent a theoretical, fully optimized (linear) model of anesthesia productivity. In this “perfect world” scenario, case volumes scale proportionally with supervision ratios, assuming continuous full concurrency, no turnover inefficiencies and perfectly synchronized operating rooms.
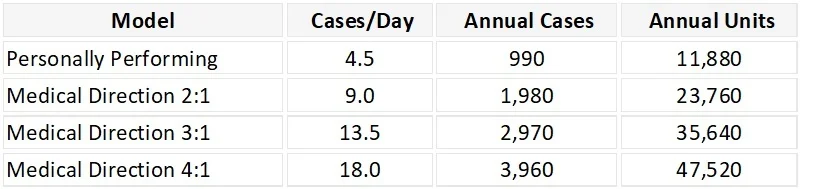
While the table above reflects clean linear scaling, real-world OR performance consistently falls below these levels because anesthesia productivity is constrained by operational factors beyond staffing ratios. Research highlights that productivity is heavily influenced by case duration, concurrency logistics and OR flow, not just staffing model. These benchmarks assume the physician receives full productivity credit for all medically directed units rather than the reimbursement split associated with medical direction billing rules. That distinction matters operationally.
Many organizations evaluate total supervised production attributable to the anesthesiologist, not simply the personally billable fraction collected under Medicare reimbursement methodology. Viewed this way, productivity increases substantially as concurrency rises.
Why Case Counts Alone Fall Short
Anesthesiologists often describe busy days by case volume, but case counts alone are poor indicators of actual productivity. Five short cataract procedures are not operationally equivalent to one complex cardiac case. Likewise, twenty GI cases may generate significantly different staffing demands than several lengthy inpatient procedures.
Case volume alone ignores:
- Procedural complexity
- Time intensity
- Staffing burden
- Concurrency management
- Non-billable physician responsibilities
That is why ASA units remain the most meaningful productivity metric in anesthesia. Units capture both procedural complexity and time, providing a far more accurate representation of clinical output and financial contribution.
The Operational Reality of Medical Direction
On paper, care team models appear highly scalable. And theoretically, they are. As supervision ratios increase, physician productivity should increase proportionally through concurrent anesthetizing locations. In reality, however, OR operations are rarely perfectly synchronized. Cases start late. Turnovers vary. Add-on procedures disrupt schedules. PACU bottlenecks create delays. Physicians move between rooms managing breaks, evaluations and operational issues that generate no direct units. The result is that many anesthesia groups never fully realize the theoretical efficiency of higher supervision ratios.
A 3:1 staffing model does not automatically produce dramatically higher productivity than a 2:1 model unless operational flow supports sustained concurrency throughout the day.
The issue is often not physician effort. It is operational alignment.
The Importance of Throughput and Case Mix
The highest-performing anesthesia groups understand that productivity is not simply determined by staffing ratios. It is driven by operational efficiency.
Groups that consistently outperform tend to:
- Align case starts effectively
- Reduce turnover delays
- Optimize room utilization
- Coordinate staffing dynamically
- Maintain consistent procedural throughput
When those systems function well, productivity scales significantly within care team models.
Case mix also plays a major role. In high-throughput environments such as GI centers and ambulatory surgery centers, anesthesiologists may participate in 20–30 cases daily through rapid turnover and short-duration procedures. Conversely, physicians handling cardiac, neuro, trauma or transplant cases may complete only one to three major procedures daily while still generating substantial unit production. This is why productivity comparisons without case mix adjustment can quickly become misleading.
Different anesthesia environments create entirely different productivity realities.
The Bottom Line
A 10,000-unit anesthesiologist may be highly productive or underperforming.
The answer depends entirely on the environment, staffing model and operational structure surrounding that production. Personally performing physicians, 2:1 medical direction models, and 3:1 care team structures are not interchangeable productivity environments.
They should not be benchmarked as though they are.
In today’s anesthesia landscape, the most important question is no longer: “How many units did the physician produce?” It is: “How efficiently did the system enable that production?”—because ultimately, anesthesia productivity is not just about provider effort. It is about operational design.